JUANITA’s STORY
Juanita was a 48-year old Hispanic female who noticed vaginal bleeding after she and her husband had intercourse. This symptom had been occurring off and on for about 6 weeks, when she decided to be evaluated at the local health department clinic. Juanita had not had a gynecologic examination or Pap smear in the past 5 years. She had been pregnant 5 times: 3 children and 2 miscarriages. She had a history of high blood pressure but was otherwise healthy. Her examination revealed a 3 cm mass on the cervix. The gynecologist obtained a biopsy of the mass which revealed squamous cell carcinoma, cancer of the cervix.
After her diagnosis, Juanita had a CT scan of her pelvis which revealed no grossly visible evidence of disease in her lymph nodes or elsewhere outside the cervix. A chest X-ray was also negative. Juanita’s gynecologic oncologist performed a radical hysterectomy which revealed a squamous cell carcinoma of the cervix with no evidence of extension into the nearby tissues, and negative surgical margins. However, she had microscopic tumor cells involving 6 out of 8 lymph nodes that were removed from the left side of the pelvis. She also had tumor cells invading along the lymphatics and blood vessels near the cervix. Juanita was referred to a radiation oncologist who recommended post-operative chemotherapy & radiation together (chemoRT). She received 5.5 weeks of treatment utilizing intensity modulated radiation therapy (IMRT), in order to minimize radiation dose to the nearby small bowel and bladder. Concurrent weekly cisplatin chemotherapy was delivered by her gynecologic oncologist. She had a difficult time during her chemoRT due to severe fatigue and diarrhea. She required admission to the hospital for 3 days near the end of treatment to receive IV fluids due to dehydration. However, within 1 month after she finished chemoRT, Juanita had recovered completely from the side effects of her treatment. Four years after completion of her chemoRT, she remains free of disease or any long-term side effects.
BASICS
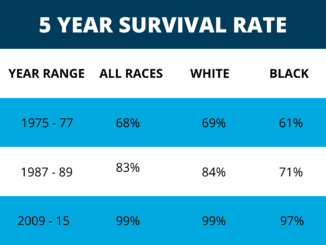
Cancer of the cervix is the most common killer of women among gynecologic cancers throughout a large part of the world. However, deaths due to cervical cancer are less common in the U.S., thanks to widespread use of the Pap test. According to the most recent NCI’s SEER Cancer Statistics Review, the 5-year survival following a diagnosis of cervix cancer for all stages combined is 70%. If the disease is localized, then the 5-year survival is 91%.
RISKS & CAUSES
The human papillomavirus (HPV) is found to be present in nearly all squamous cell cancers of the cervix. Infection with HPV is the leading risk factor for development of cervical cancer. Two strains of HPV, type 16 & 18, are the most often associated with cervical cancer. The two vaccines that have been produced to prevent cervical cancer are designed to protect against these strains of HPV. Vaccination is approved in the U.S. for females ages 9 through 26 (& now males also!). The available vaccines don’t eliminate HPV in a woman who’s already infected. The majority of women who develop HPV infection will clear it on their own within 1-2 years and will NOT develop cervical cancer. Activities that put women at risk for HPV infection (such as having multiple sexual partners) also place them at risk for cervical cancer. Much to the surprise of many young women, tobacco smoking also has been clearly linked to an increased risk for the development of cervical cancer. Therefore, most (but not all) of the risk factors for cervical cancer can be modified or changed by women who make the effort to protect themselves.
SIGNS & SYMPTOMS
The classic symptoms of cervical cancer are vaginal bleeding, most notably following intercourse, called post-coital bleeding. Some women may visit their gynecologist with complaints of pelvic pain without bleeding. Those patients who present with significant symptoms and are found to have more advanced cancer, usually haven’t had routine gynecological exams including Pap testing. The Pap test is an extremely effective screening tool for the prevention and/or early detection of cervical cancer.
DIAGNOSIS
Most women are diagnosed with cervical cancer following examination and biopsy of the cervix by their gynecologist. Patients should then be referred to a gynecologic oncologist, a surgeon specializing in the care of patients with gynecologic cancers. Roughly 80% of cervical cancers are squamous cell carcinomas.
STAGING
Historically, the primary staging system for cervical and other gynecologic cancers was based on the FIGO system. Patients with very early stage disease have smaller cancers limited to the cervix. Locally advanced disease includes large cervical tumors that invade into the nearby tissues within the pelvis, as well as those that involve pelvic lymph nodes.
TREATMENT
Patients with early stage cervical cancer should be treated surgically by a gynecologic oncologist. The standard surgical procedure is called a radical hysterectomy, which differs from what most people think of as a hysterectomy. In addition to the uterus, the fallopian tubes, ovaries, parametria (tissue on the sides of the cervix), ligaments and tissues that support the uterus, and upper portion of the vagina are all surgically removed by the gynecologic oncologist. Cure rates exceed 80% overall. Potential acute side effects of radical hysterectomy include bleeding, infection, urinary or bowel injury, sexual dysfunction, and rarely life-threatening blood clots to the lungs.
Certain patients will benefit from post-operative radiation therapy (RT) to their pelvis. These groups include patients with cancer cells at the edge of where the surgeon removed the tumor (positive margins), involvement of lymph nodes, parametria, or within lymphatic and vascular channels. Post-operative concurrent chemoRT improves survival over RT alone and is the standard of care for these patients at high risk of cancer returning within the pelvis.
Locally advanced cervical cancer is fortunately becoming much less common throughout most of the U.S. due to the widespread use of Pap testing. The standard treatment for these patients is concurrent chemoRT. This regimen usually includes both external and internal RT. External RT is delivered over roughly 5 weeks of daily treatment. The internal RT may be delivered in the hospital over 2-3 consecutive days usually after completion of external RT, or as an outpatient once per week beginning midway through the treatment course. Medications are given to minimize discomfort.
The most frequent acute side effects of RT to the pelvis include irritation of bladder and bowel causing frequency and/or discomfort with urination or bowel movements. Fatigue and decreased blood counts are also common side effects of chemoRT in this setting. Approximately 5-10% of women will have chronic bladder or bowel problems that affect their quality of life long-term. Rarely, RT may cause permanent bowel or bladder injury requiring surgery to repair. There is also a small but real risk of vaginal stenosis, scarring at the top of the vagina, that may cause pain. The risk of this scarring can be minimized by using a medical dilator to keep the tissue healthy.
Cisplatin is the chemotherapy drug most commonly delivered during RT, usually in low doses once per week. The common acute side effects include decreased blood counts, poor appetite, fatigue, and nausea and vomiting (which are usually very well controlled on current anti-nausea medicines). Uncommon but serious long-term risks of cisplatin include possibility of damage to the kidneys and nerves, as well as loss of high frequency hearing.
Proudly WWW.PONIREVO.COM